 |
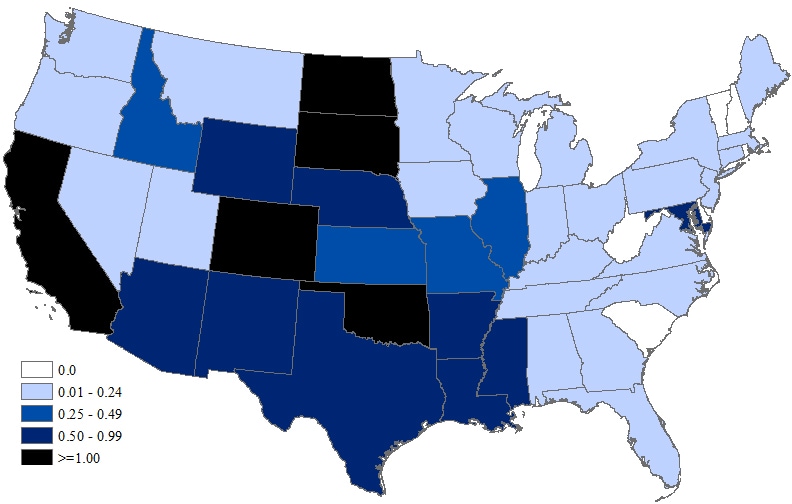
| Regions Where Aedes Mosquitoes Are Endemic |
|
#10,890
The news this week that an
imported case of Zika arrived in Harris County, Tx is only the latest in a steady stream of arbovirus infected travelers who arrive in the United States pretty much on a daily basis. Zika is a new threat, but for years we've had imported cases of Dengue, Malaria, and more recently - Chikungunya - to deal with.
In 2009, Dengue fever returned to Florida after six decades without a locally acquired case (see MMWR: Dengue Fever In Key West), and since that time we've seen sporadic outbreaks in South Florida, Texas, and most recently Hawaii.
That
MMWR report described Florida's vulnerability to Dengue as follows:
The environmental and social conditions for dengue transmission have long been present in south Florida: the potential for introduction of virus from returning travelers and visitors, the abundant presence of a competent mosquito vector, a largely nonimmune population, and sufficient opportunity for mosquitoes to bite humans.
The same mosquito vectors (
Aedes) that transmit Dengue also can transmit Chikungunya, (and Zika) and so this assessment is likely valid for all three arboviruses. In late 2013, soon after Chikungunya began to spread rapidly across the Caribbean, the
CDC issued a HAN Advisory On Recognizing & Treating Chikungunya Infection for clinicians in the United States.
True to form, in 2014 Florida reported 459 International Travel-Associated Chikungunya Fever Cases and 11 cases of locally acquired CHKV (cite Fl. DOH). Nationally, in 2014, the United States reported roughly 2,800 imported cases.
We got lucky in that CHKV failed to establish a foothold that year, but past failures are no guarantee that our luck will hold forever. Now, CHKV and Dengue are joined by a new threat - Zika - and 2016 could be a very challenging year for mosquito control in Florida, and across the country.
The State of Florida published it's
2015 Arbovirus re-cap last week, and it it we find that more than 200 international travelers with either Dengue (
83 cases), Chikungunya (
73 cases), or Malaria (
53 cases) were reported to the Health Department last year.
As 80% of Dengue and Chikungunya cases are believed asymptomatic (or produce only mild symptoms), one can assume these reported cases are only subset of the total.
Each one of these infected travelers has the potential to provide a blood meal to an
Aedes mosquito, who could then spread the virus
(or an Anopheles mosquitos with the malaria parasite) to others. Granted, unless conditions are ideal, it may take many repeated introductions of these diseases over years before one becomes established in the United States.
But as we saw with West Nile Virus, which only arrived in 1999, it can happen much quicker than we ever imagined. In 2015 WNV killed at least 119 Americans.
 |
| 2015 Neuroinvasive WNV |
WNV has an advantage in that it has a sylvatic cycle (
birds to mosquitoes)
. Human infection is basically a result of incidental
collateral damage (see graphic below).
Zika, Dengue, and Chikungunya - at least outside of Africa and Asia - have no known non-human animal reservoirs, which means they have a harder time becoming endemic. But when enough people become infected, these viruses are sometimes able to sustain themselves in an Urban Cycle, where transmission is strictly human-to-mosquito-to human.
The conventional wisdom, however, says that (
at least in colder climes), the virus must be reintroduced each year as infected mosquitoes die off during the winter.
Possibly throwing a wrench into that idea is a recent study (Feb 2015) suggesting that some mosquitoes may be capable of vertical transmission of some arboviruses (see
Natural transovarial transmission of dengue virus 4 in Aedes aegypti from Cuiabá, State of Mato Grosso, Brazil), allowing new generations of mosquitoes to be born already carrying the disease. The authors write:
The findings reported in this study demonstrate that natural transovarial infection by DENV-4 is occurring in Ae. Aegypti in Cuiabá with a relatively high MIR index, which favors the birth of mosquitoes already infected with DENV at the beginning of epidemics. This mechanism may be responsible for virus maintenance during interepidemic periods, especially in critical areas with elevated mosquito density and human disease incidence.
There are a lot of factors at work - a lot of unknowns - but the upshot of all of this is that Zika, Chikungunya, and Dengue all have at least some potential to spark (
likely regional, and limited) epidemics in the contiguous United States.
Maybe not this year, or next, but the requisite ingredients are all here.
A continual and growing influx of infected travelers and a competent mosquito vector. Just add in the right weather conditions, and a tightly packed urban population - and you have a recipe for an outbreak.
And it isn't just the United States at risk.
Europe, Australia, and Japan have all reported arbovirus outbreaks in regions that haven't reported mosquito borne diseases for decades. A few months ago, in
ECDC Vector Maps: Invasive Ticks, Mosquitoes & Sand Flies we looked at numerous places in Europe where these diseases might become established once again.
While the United States and Europe have waged very successful wars against mosquitoes over the past 70 years, many of our mosquito control tools are starting to lose effectiveness around the world.
The WHO warns:
Resistance is known to affect all major malaria vector species and all four recommended classes of insecticides. Since 2010, a total of 60 countries have reported resistance to at least one class of insecticide, with a total of 49 of those countries reporting resistance to two or more classes. However, our understanding of the extent of the problem is incomplete, because:
- many countries do not carry out adequate routine monitoring for insecticide resistance in local vectors; and
- monitoring data are often not reported in a timely manner.
A 2014 PLoS One Study
Insecticide Resistance Status of United States Populations of Aedes albopictus and Mechanisms Involved noted some pockets of mosquitoes resistant to DDT and malathion in both Florida and New Jersey. They wrote:
This study showed standard larvicides and pyrethroids used for mosquito control are still effective against USA populations of Ae. albopictus, but it also demonstrates the importance of research on insecticide resistance and the constant need to develop new tools, new insecticides, and innovative strategies to prevent the development of insecticide resistance in these critical vectors of human diseases.
And in 2010, in
From the `Nature Bats Last’ Dept we looked at reports that one of our most effective mosquito repellents -
DEET, or
N,N-Diethyl-m-toluamide (
a name that, for some reason, never really caught on with the public) - may be losing some effectiveness. A story I followed up with in 2013 with
PLoS One: Mosquitoes Less Deterred By DEET After Previous Exposure.
All signs that - with a growing array of mosquito-borne threats in the wings - we can't afford to take the mosquito threat lightly anymore. Not even in places that have been considered
`safe' from these types of diseases for decades.



















 src="https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEh4zgoKkY5esDyGDfXmhp5tz0W8H2jEgsRJx2wm9317hpr6CTdO8i4DPQj5mF-OAprw6GVcNt84Pt9Yp5U6XEz5h_pAP7azclFEO7kSUzDjr31IvLdzT01usqHnjVk1bBWsqpHQX6G4AIU/s1600/Photo0783.jpg" />
src="https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEh4zgoKkY5esDyGDfXmhp5tz0W8H2jEgsRJx2wm9317hpr6CTdO8i4DPQj5mF-OAprw6GVcNt84Pt9Yp5U6XEz5h_pAP7azclFEO7kSUzDjr31IvLdzT01usqHnjVk1bBWsqpHQX6G4AIU/s1600/Photo0783.jpg" />












