
 | |
| Credi MMWR |
#11,008
The CDC has published, late this afternoon, an extensive MMWR review of local acquisition of the Zika virus in the U.S. Territory of Puerto Rico - to date involving 30 individuals - including one pregnant woman.
The review, charts, and map are far too large to excerpt here effectively, so I'll simply direct my readers to follow the link. I have excerpted the summary.
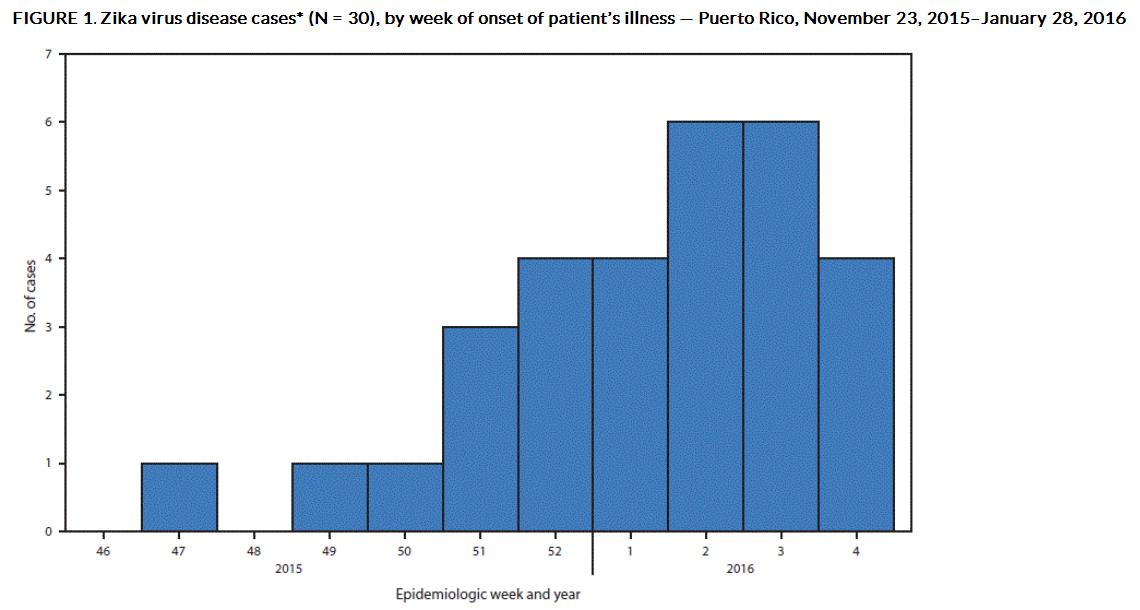
Local Transmission of Zika Virus — Puerto Rico, November 23, 2015–January 28, 2016
FEBRUARY 12, 2016
On December 31, 2015, the Puerto Rico Department of Health reported the first locally acquired case of Zika virus disease in a jurisdiction of the United States in a patient from southeastern Puerto Rico. Zika virus is expected to continue to spread throughout the territory, and the 3.5 million residents of Puerto Rico, including approximately 43,000 pregnant women per year, are at risk for Zika virus infection.
Early Release / February 12, 2016 / 65(6);1–6
Dana L. Thomas, MD1,2; Tyler M. Sharp, PhD3; Jomil Torres, MS1; Paige A. Armstrong, MD4; Jorge Munoz-Jordan, PhD3; Kyle R. Ryff, MPH1; Alma Martinez-Quiñones, MPH5; José Arias-Berríos, MD6; Marrielle Mayshack1,7; Glenn J. Garayalde, MD8; Sonia Saavedra, MD, PhD8; Carlos A. Luciano, MD6; Miguel Valencia-Prado5; Steve Waterman, MD3; Brenda Rivera-García, DVM1
Summary
What is already known about this topic?Zika virus emerged in the Region of the Americas in mid-2015, and since then, outbreaks have occurred in multiple South American and Caribbean countries and territories. Zika virus infection appears to be related with increased risk for fetal microcephaly and Guillain-Barré syndrome.
What is added by this report?The first locally acquired case of Zika virus disease in Puerto Rico was identified in early December 2015. During the subsequent months, 29 additional laboratory-confirmed cases have been detected, including in one pregnant woman and in a man with Guillain-Barré syndrome.
What are the implications for public health practice?Clinicians in Puerto Rico and other clinicians evaluating patients with recent travel to Puerto Rico should report all cases of suspected Zika virus disease to public health authorities. Residents of and visitors to Puerto Rico should strictly follow steps to avoid mosquito bites including using air conditioning or window and door screens when indoors, wearing long sleeves and pants, using permethrin-treated clothing and gear, and using insect repellents. When used according to the product label, Environmental Protection Agency-registered insect repellents are safe for pregnant women.
















 src="https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEh4zgoKkY5esDyGDfXmhp5tz0W8H2jEgsRJx2wm9317hpr6CTdO8i4DPQj5mF-OAprw6GVcNt84Pt9Yp5U6XEz5h_pAP7azclFEO7kSUzDjr31IvLdzT01usqHnjVk1bBWsqpHQX6G4AIU/s1600/Photo0783.jpg" />
src="https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEh4zgoKkY5esDyGDfXmhp5tz0W8H2jEgsRJx2wm9317hpr6CTdO8i4DPQj5mF-OAprw6GVcNt84Pt9Yp5U6XEz5h_pAP7azclFEO7kSUzDjr31IvLdzT01usqHnjVk1bBWsqpHQX6G4AIU/s1600/Photo0783.jpg" />











